Executive abstract
This research was conducted to assess access to health services situation in urban and rural areas of Afghanistan. The results, based on a survey of 1,136 citizens across 32 provinces, indicate significant differences between urban and rural areas in terms of access, quality of services, and availability of medicines. Findings suggest that rural residents face greater challenges in obtaining quality health services.
Key findings
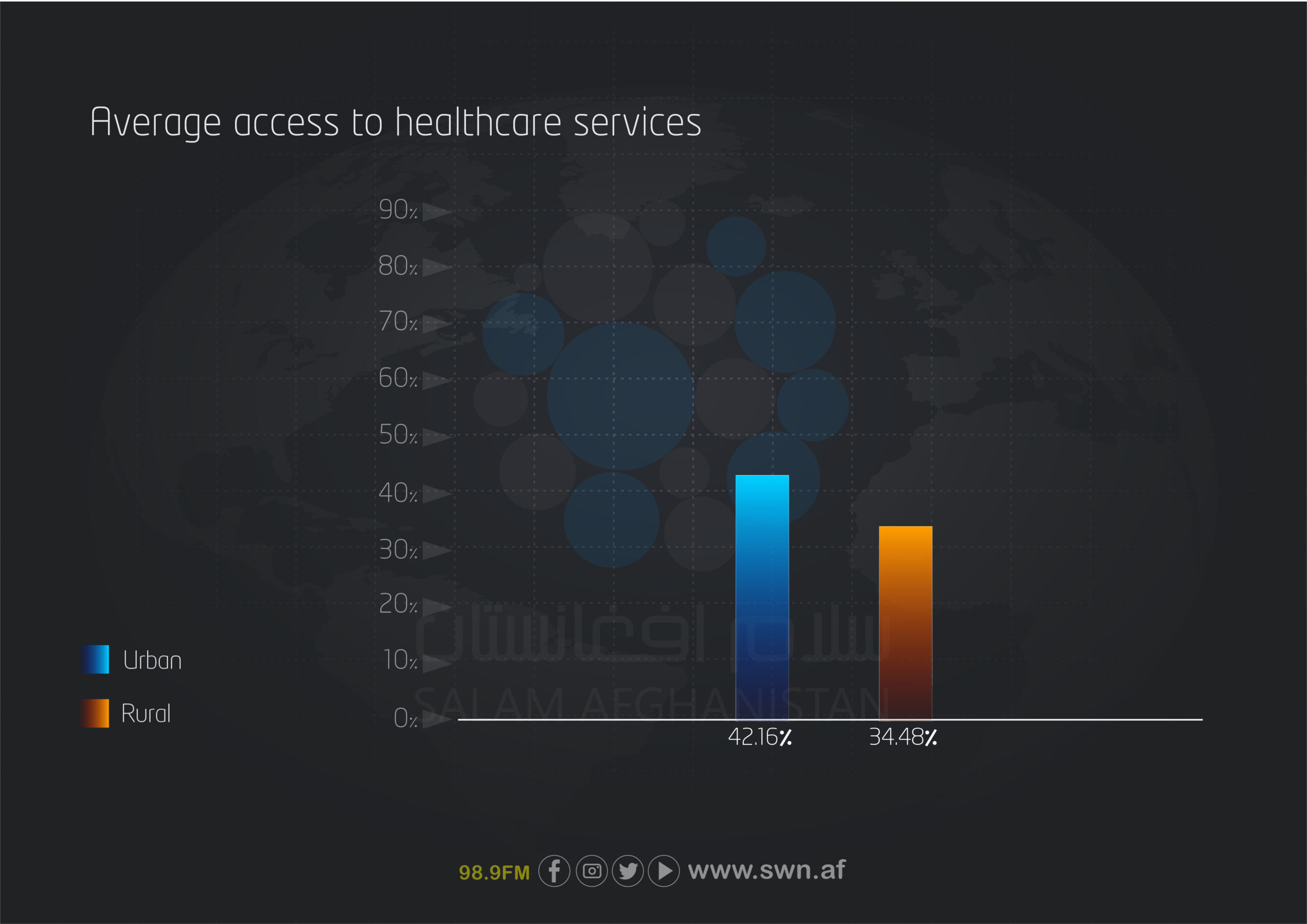
- Among 100% of rural participants, 34.48% reported access to health services, whereas in urban areas this figure was 42.16%.
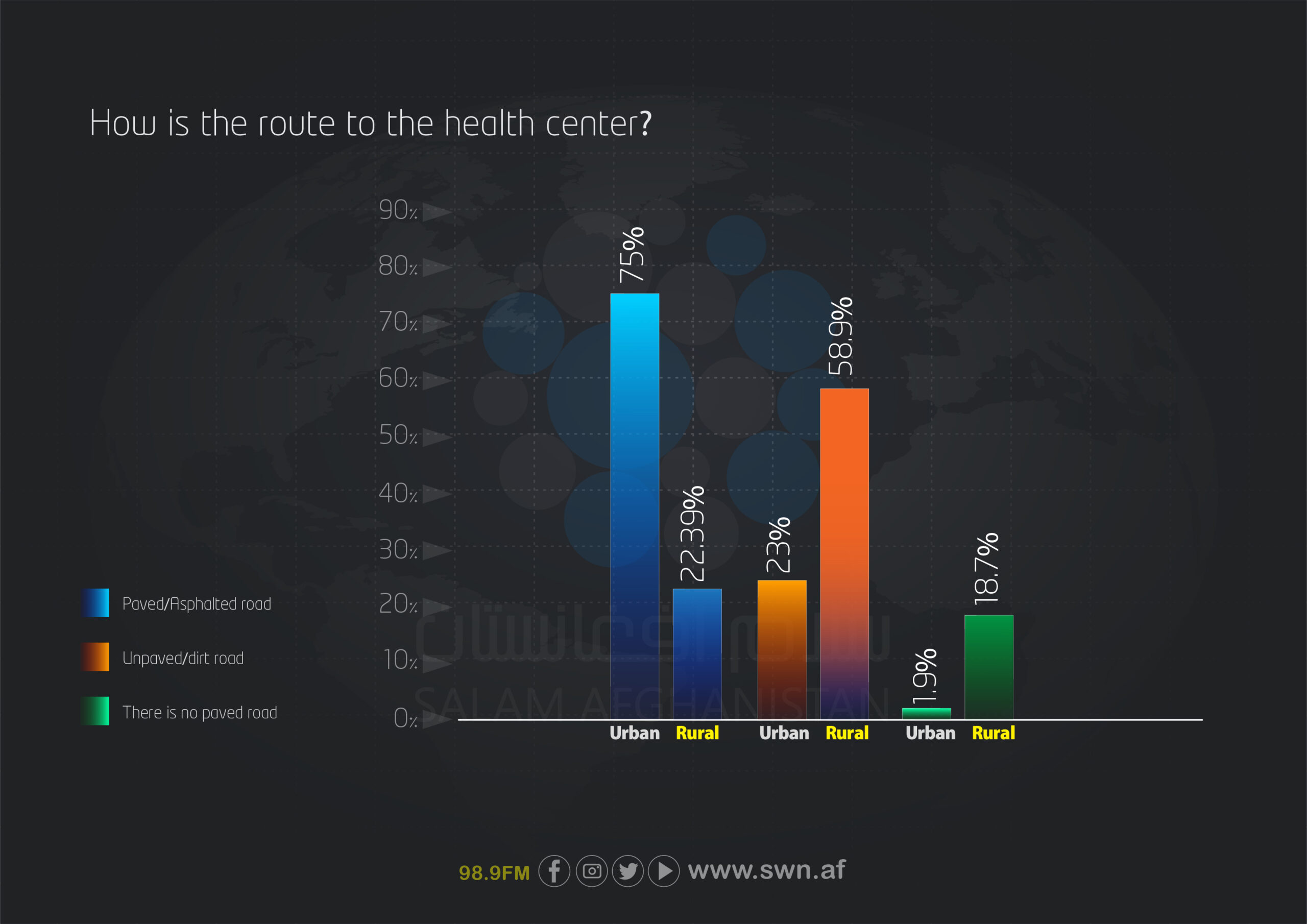
- 75% of urban residents reported that the roads were smooth and paved, compared to only 22.39% of rural residents.
- 4% of rural participants expressed concern over the low quality of health services.
Survey objectives
General objective: To assess the situation of access to health services and identify gaps between urban and rural areas in Afghanistan.
Specific objectives:
- To examine the extent and manner of people’s access to health centers.
- To evaluate the quality of services provided in health centers.
- To assess the situation regarding the availability of medicines.
- To identify geographical and infrastructural barriers to accessing health services.
- To compare the situation between urban and rural areas.
Statistical population and sample
- Statistical population: Residents of urban and rural areas of Afghanistan
- Sample size: 1,136 individuals, including:
- Urban areas: 676
- Rural areas: 460
Data collection tool
A structured questionnaire with 10 main questions covering:
- History of visits to health centers
- Type and accessibility of services
- Quality of services received
- Status of medicines
- waiting times and geographical distance
- Transportation conditions
- awareness activities.
Analysis method
- Descriptive statistics (frequency and percentage)
- Comparative analysis between urban and rural areas
Research period: April to August 2025
Publication date: July–August 2025
Definition of health services: Health services refer to a set of actions, facilities, and care provided to maintain, improve, and restore individuals’ health. These services may include prevention, diagnosis, treatment, rehabilitation, and supportive care and are delivered through medical centers, pharmacies, health centers, care teams, and public health programs.
Limitations of the study
- Limited access to some remote areas due to complex geography and time constraints.
- Lack of access to comprehensive historical data.
- Limited resources to cover all districts fully.
Overview of the assessment of the health services situation in urban and rural areas of Afghanistan
Report summary
Salam Watandar conducted a survey among 1,136 citizens across 32 provinces to assess the access situation to healthcare services in urban and rural areas. Based on the collected data from 10 different indicators, the survey revealed significant differences in service quality, access to medicines, physical paths accessibility, and health awareness supports between urban and rural populations.
Based on the findings of this report, the average access to health services is 34.48% among rural residents and 42.16% among urban residents. This indicates a low level of public access to healthcare in the country, with the difference being that rural residents not only have lower access levels, but they are also harmed by poorer service quality due to a lack of facilities, geographical distances, and weak infrastructure. Such inequalities in access and quality can exacerbate health problems in rural areas and widen the health gap between urban and rural populations.
The survey results show that the availability of health services in villages is significantly weaker compared to provincial centers. Residents of rural areas often have to spend over an hour to an entire day to reach healthcare centers. Unpaved, rough, and, in some cases, impassable roads pose serious obstacles to quick and timely access to healthcare, particularly in emergencies. Moreover, rural residents face a severe shortage of medicines and basic medical equipment. In urban areas, patients also frequently wait more than an hour to receive services, which reflects the system’s limited capacity, inefficiency of the health system, and lack of effective management in service delivery. These conditions further exacerbate inequalities in access and quality, leaving rural residents more vulnerable and at higher risk.
The absence of regular and structured awareness programs is another factor contributing to the gap in healthcare access between rural and urban populations. Residents from both groups reported that no awareness teams or educational campaigns have been conducted in their areas for over a year. This lack of awareness-raising, especially regarding prevention, basic care, and recognition of disease symptoms, has kept public health awareness at a very low level.
Furthermore, the lack of variety in healthcare centers limits the types of services available. In rural areas, people rely solely on governmental centers and, due to the absence of private healthcare options, have no alternatives or competitive choices. This monopoly not only lowers the quality of services but also reduces the motivation to improve performance in existing centers. In urban areas, although access to private centers is more readily available, high costs and insufficient oversight pose serious challenges for patients. Overall, the lack of effective awareness programs and the absence of diversity in service provision weaken service quality, reduce patient satisfaction, and increase vulnerability—particularly in rural areas.
Data analysis based on tables
Demographic characteristics of respondents
Overall report
Salam Watandar conducted a survey among 1,136 citizens across 32 provinces to assess the access situation to healthcare services in rural and urban areas of Afghanistan. Based on data collected from 10 different indicators, the survey examines and compares the accessibility situation, quality, satisfaction, and challenges of using healthcare services among residents of urban and rural areas. The results show that, although visits to healthcare centers are relatively active in both groups, there are significant differences in service quality, access to medicines, physical accessibility, and awareness support between the two populations. The findings highlight the need to improve infrastructure and strengthen health awareness systems in rural areas.
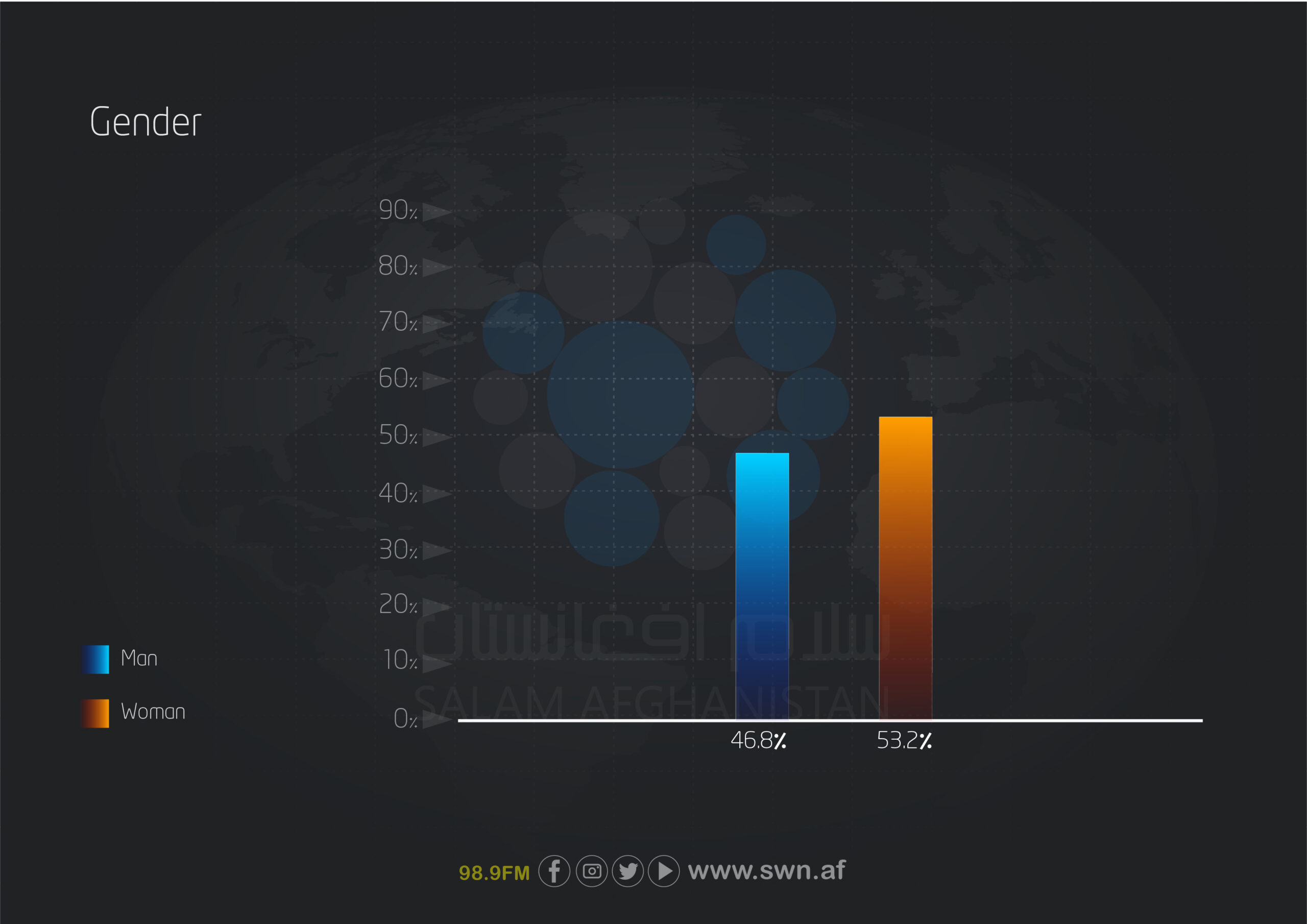
This survey was conducted among 1,136 individuals across 32 provinces of Afghanistan, of whom 604 (53.2%) were women and 532 (46.8%) were men.
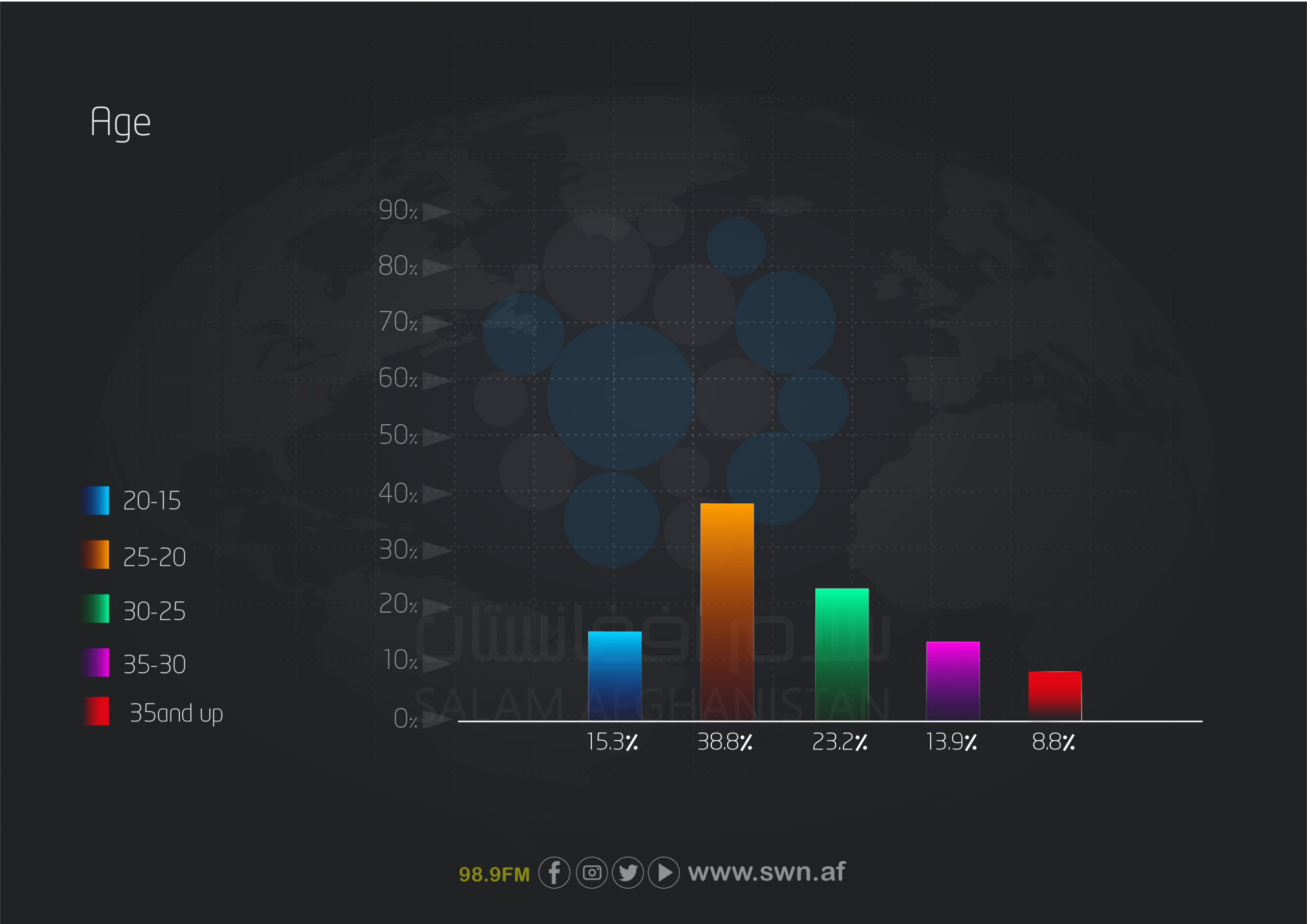
The largest age group was 20 to 25 years, representing 38.8% of participants, followed by those aged 25 to 30 years (23.2%), 15 to 20 years (15.3%), 30 to 35 years (13.9%), and 35 years and older (8.8%). This indicates that young people have more limited access to healthcare services.
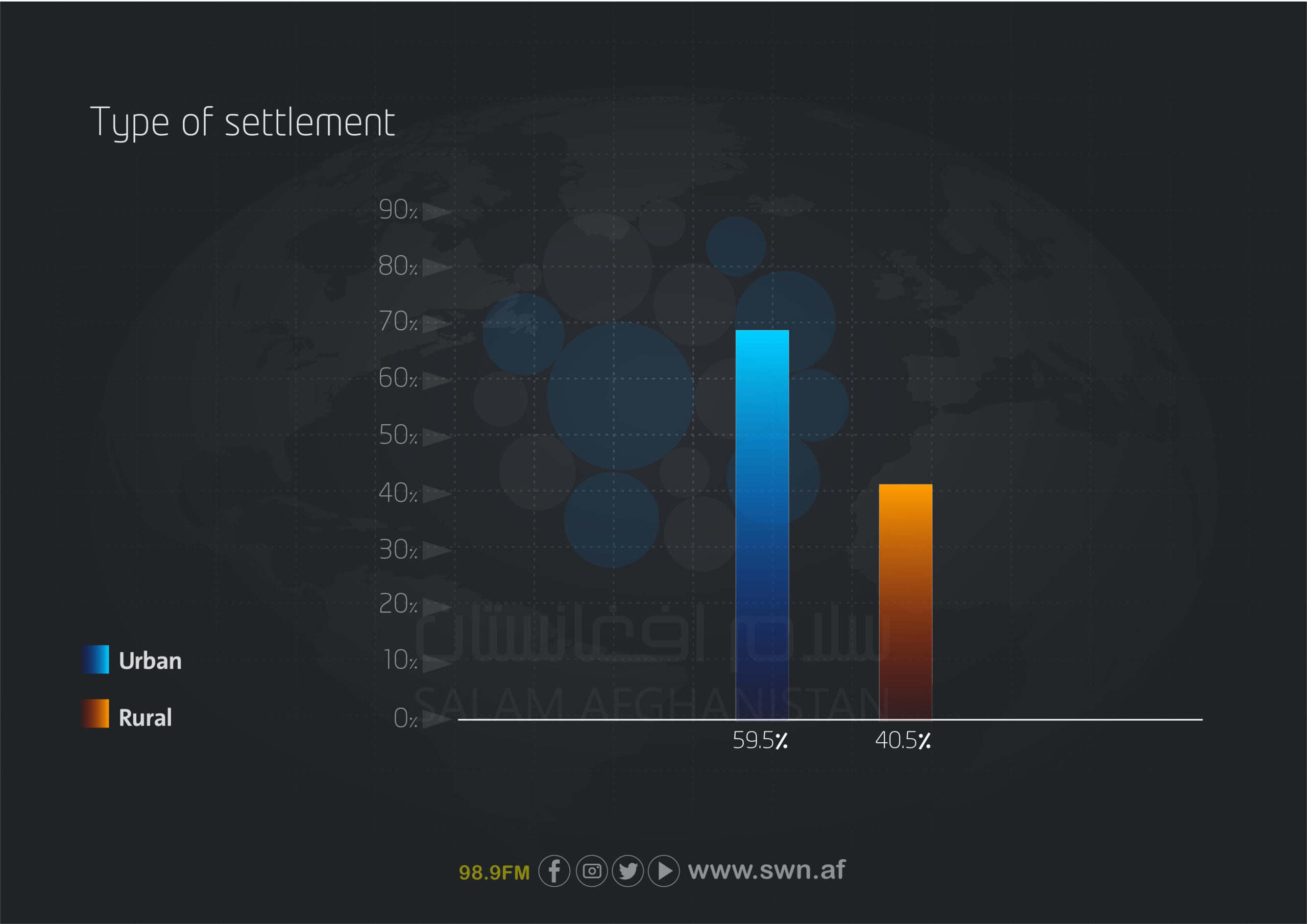
This report also examined the participants’ living environment. Of the total, 676 individuals (59.5%) were urban residents, while 460 individuals (40.5%) were rural residents.
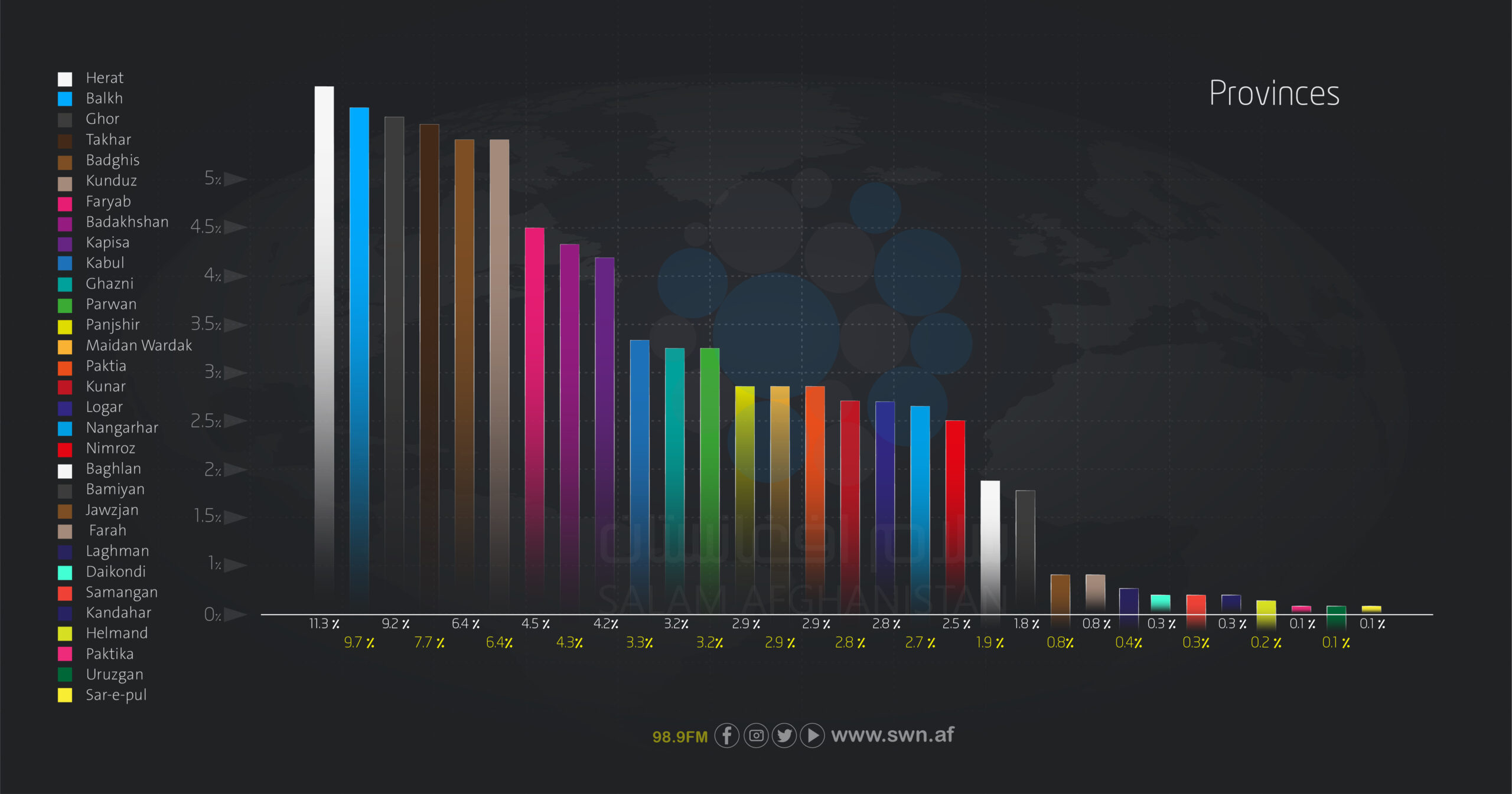
The respondents participated from 32 provinces, with the highest numbers from Herat (128 individuals, 11.3%), Balkh (110, 9.7%), Ghor (104, 9.2%), Takhar (87, 7.7%), and Badghis (73, 6.4%). Provinces with the fewest respondents were Sar-e Pul, Uruzgan, and Paktika, each contributing only one participant (0.1%).
Based on the responses of the survey participants, the average access to healthcare services is 34.48% among rural residents and 42.16% among urban residents.
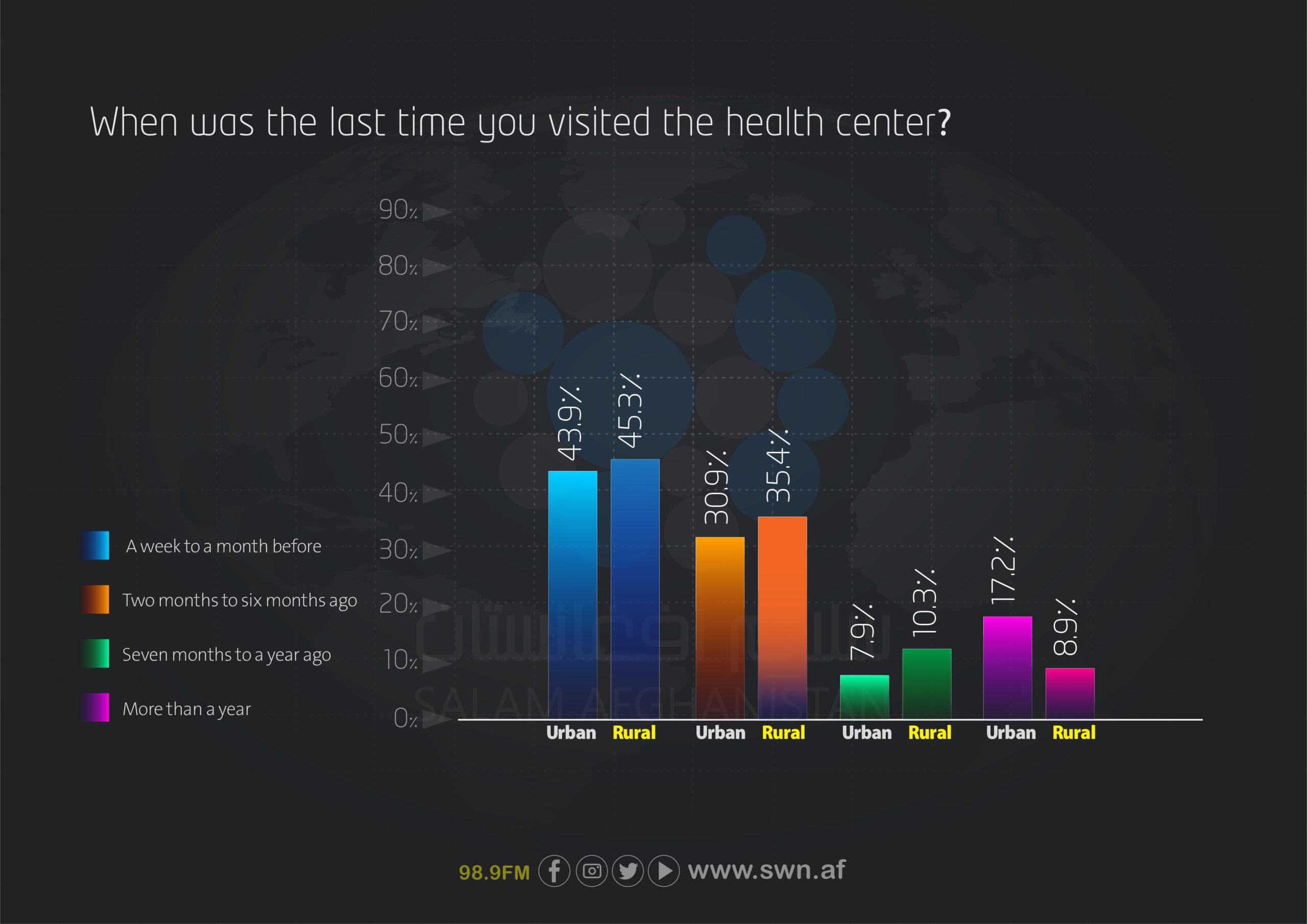
The frequency of visits to healthcare centers in the past month is notable in both urban and rural groups. Among urban respondents, 43.9% visited healthcare centers within the past week to month, while 45.3% of rural respondents did so. Additionally, 30.9% of urban residents and 35.4% of rural residents visited healthcare centers within the past two to six months. In contrast, the percentage of individuals whose last visit was over a year ago was 17.2% in urban areas and 8.9% in rural areas, indicating that regular visits to healthcare centers are less frequent in cities than in rural areas.
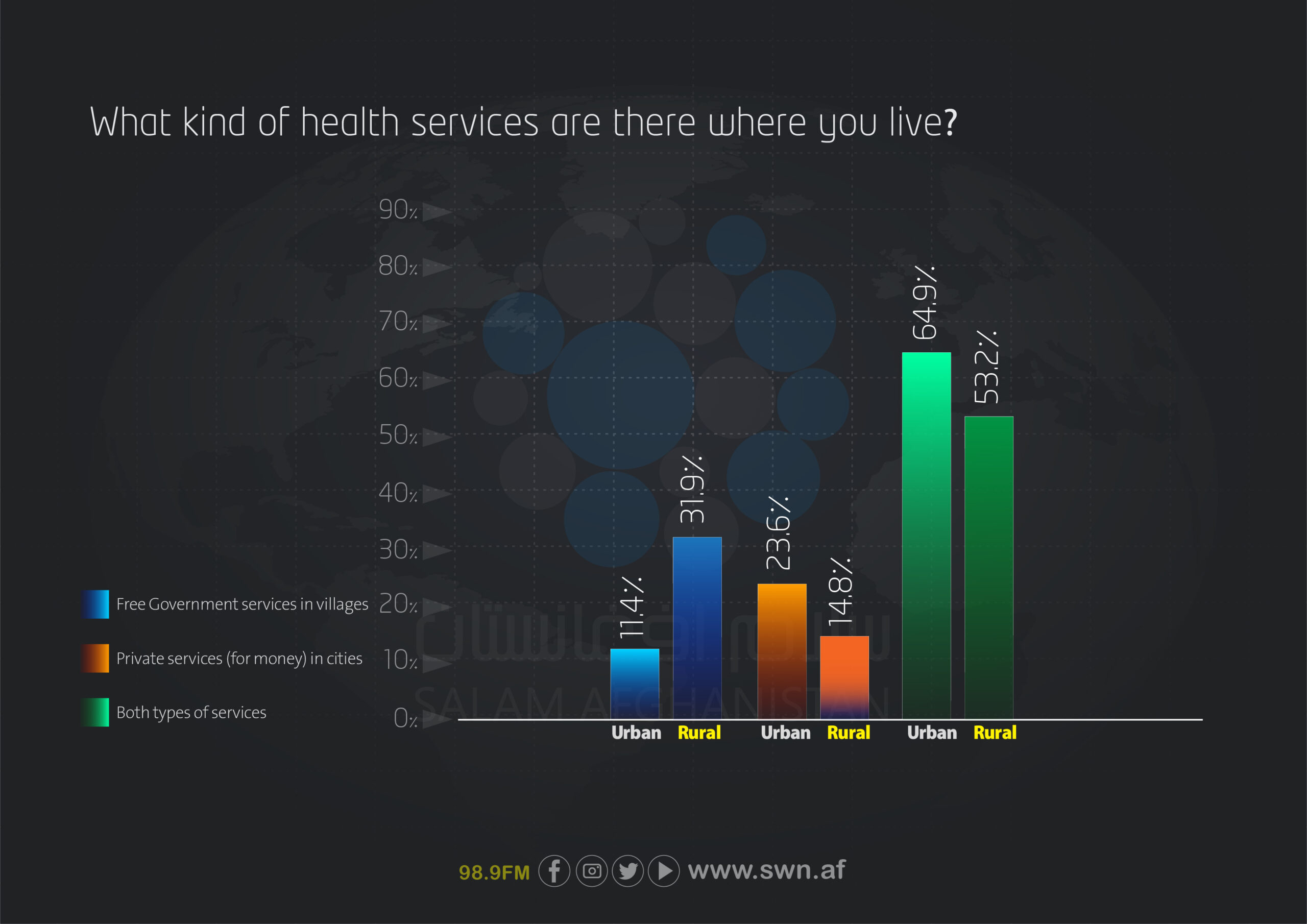
Access to healthcare services at the place of residence also differs between urban and rural areas. In cities, 64.9% of respondents reported having access to both types of healthcare services (private and governmental), whereas this figure is 53.2% in rural areas. Governmental services are more important in rural areas, with 31.9% of residents relying on them, compared to only 11.4% in urban areas. In contrast, the use of private services is higher in cities (23.6%) than in rural areas (14.8%).
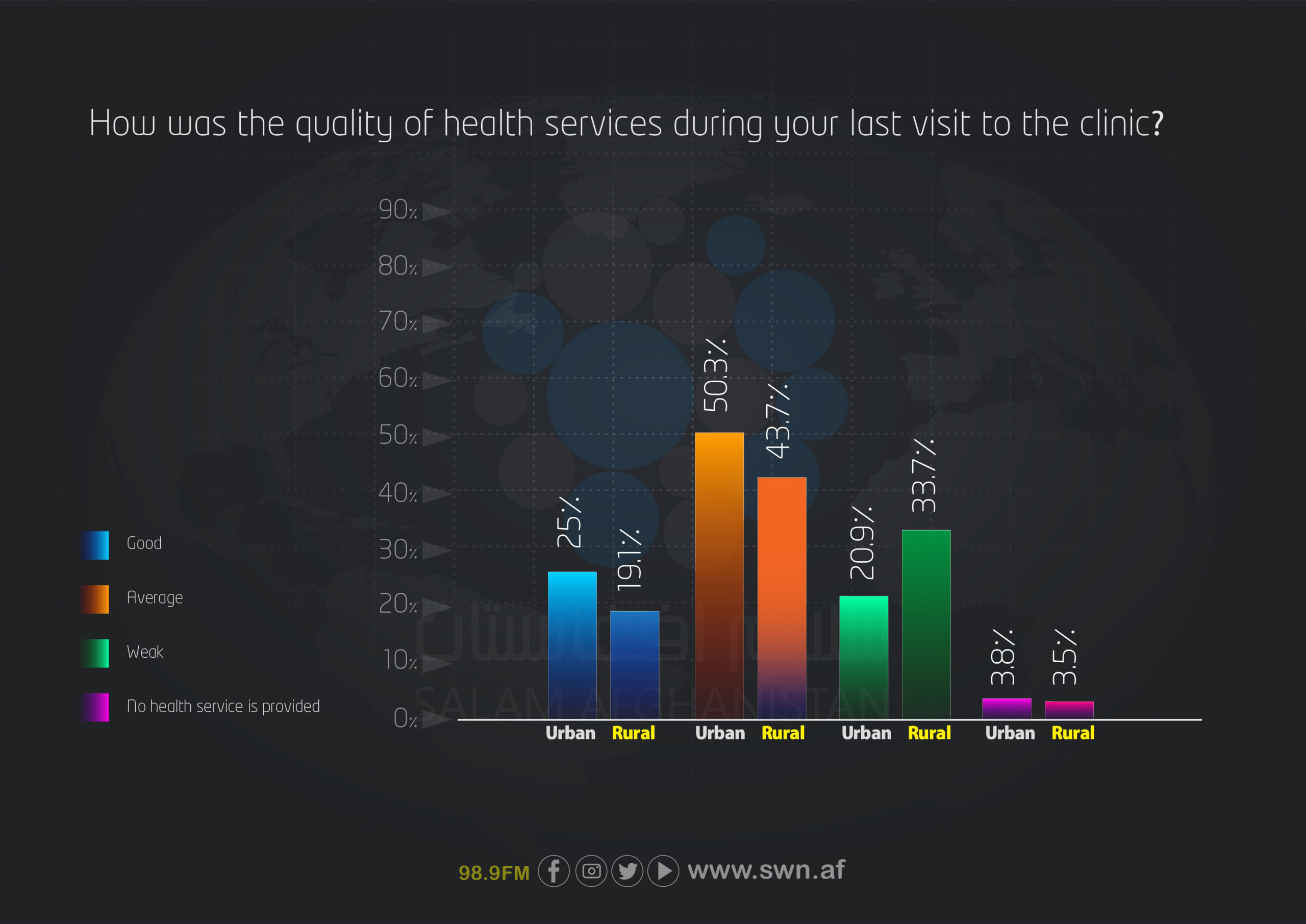
The quality of healthcare services received during the most recent visit was also assessed. Among urban respondents, 25% rated the quality of services as good, compared to 19.1% of rural respondents. The majority of participants—50.3% of urban residents and 43.7% of rural residents—considered the services to be of average quality. Poor service quality was reported more frequently in rural areas (33.7%) than in urban areas (20.9%). The percentage of respondents who stated that services were not provided at all was below 4% in both groups.
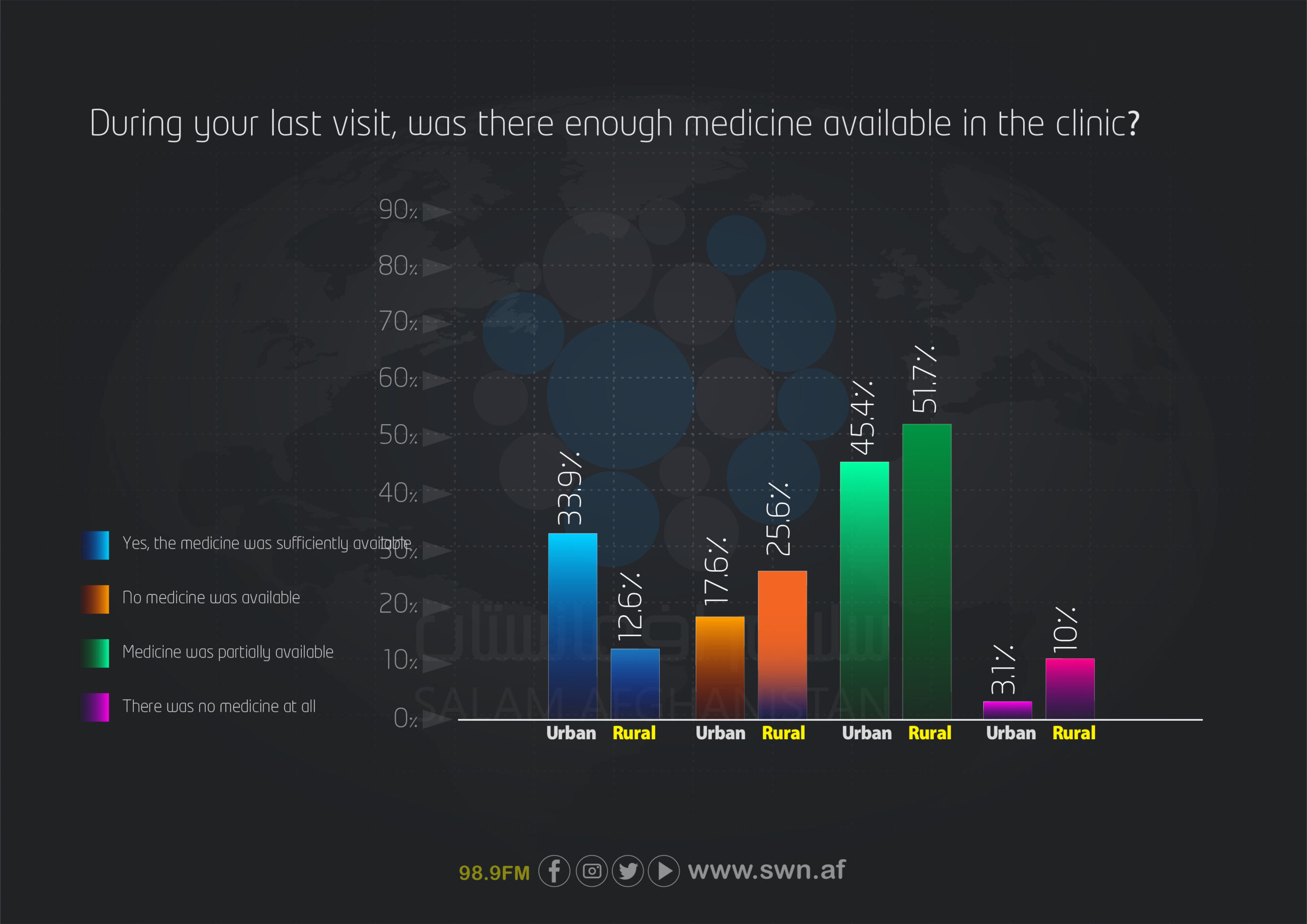
Access to medicines during visits to healthcare centers also shows notable differences. In cities, 33.9% of respondents reported that medicines were sufficiently available, whereas this figure is only 12.6% in rural areas. Medicines were somewhat available in both areas, representing the highest proportion—45.4% in cities and 51.7% in rural areas. Complete unavailability of medicines was also more pronounced in rural areas (10%) compared to cities (3.1%).
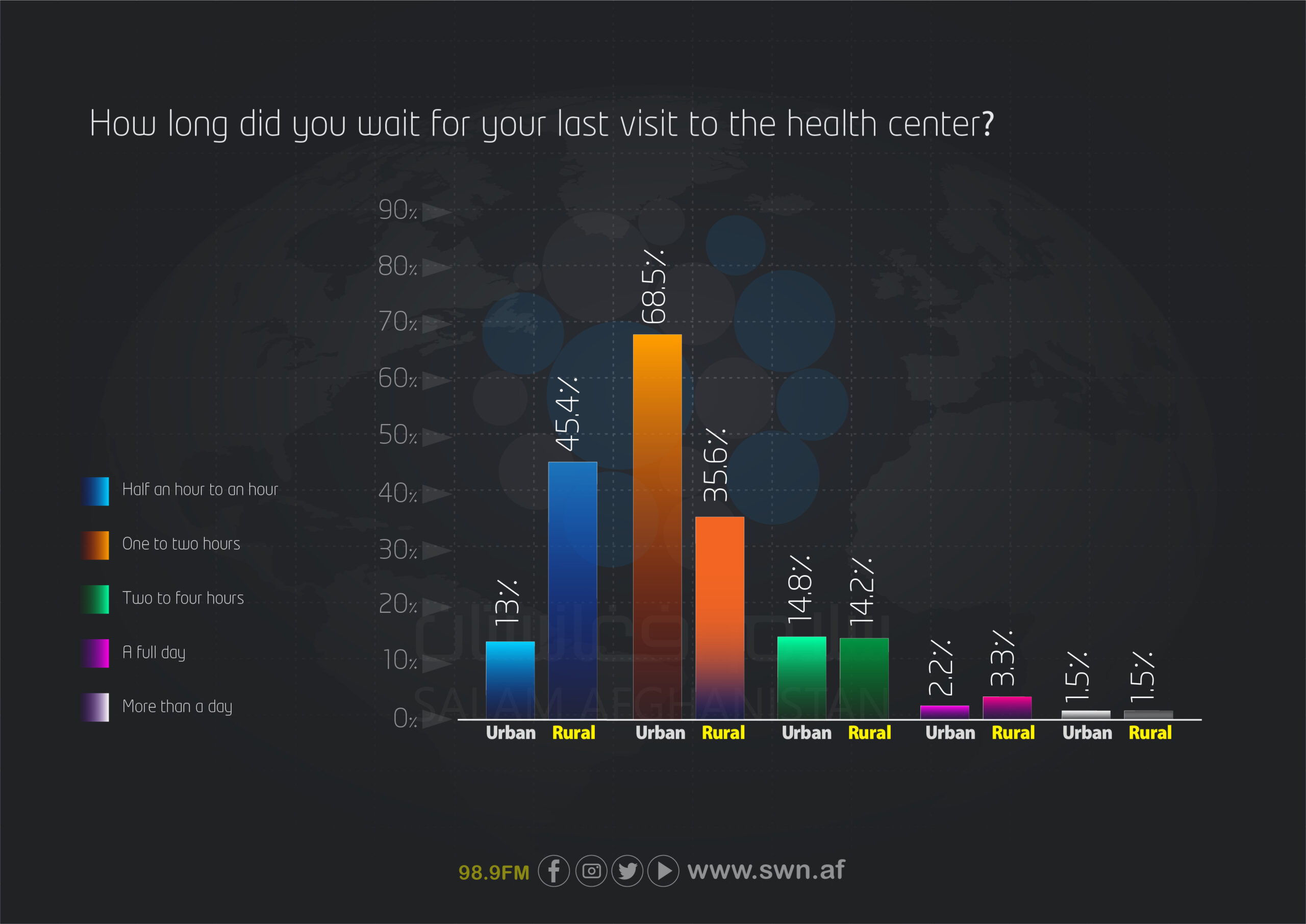
Regarding waiting times at healthcare centers, the data show that 68.5% of urban visitors waited one to two hours, whereas in rural areas, 45.4% waited only half an hour to one hour. Longer waiting times (two hours to one day) were reported less frequently in both areas; however, they were slightly higher in rural areas.
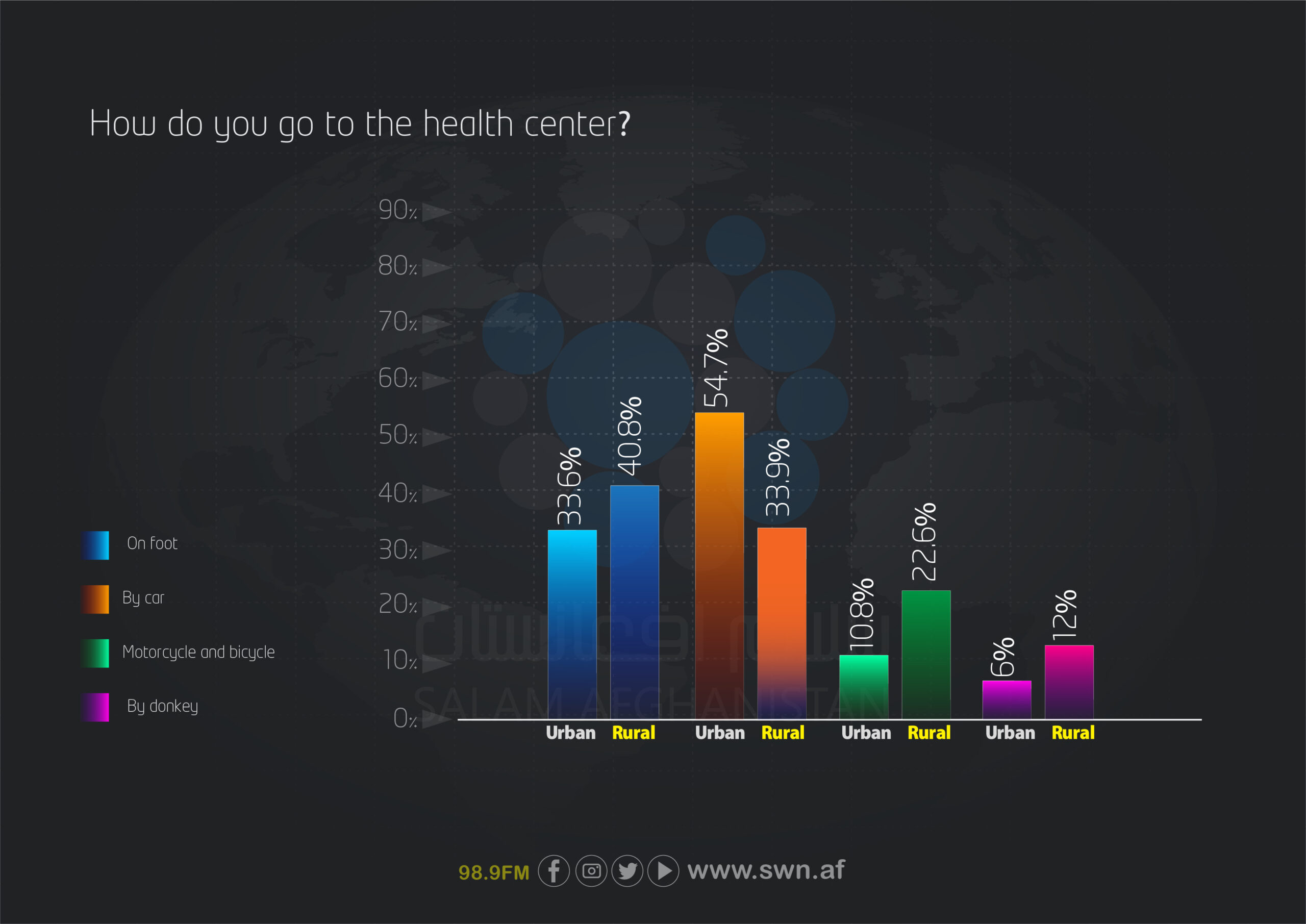
Modes of transportation to healthcare centers also differ. In cities, the majority of respondents (54.7%) travel to healthcare centers by car, whereas in rural areas, most people (40.8%) go on foot. The use of motorcycles and bicycles is more than twice as common in rural areas (22.6%) compared to cities (10.8%), and a small minority in both areas use animals for transportation.
The condition of roads leading to healthcare centers was significantly better in urban areas, where 75% of respondents reported paved and smooth routes. In contrast, only 22.39% of rural respondents had similar conditions. A majority of rural residents (58.9%) reported unpaved and rough roads, and 18.7% described their routes as impassable.
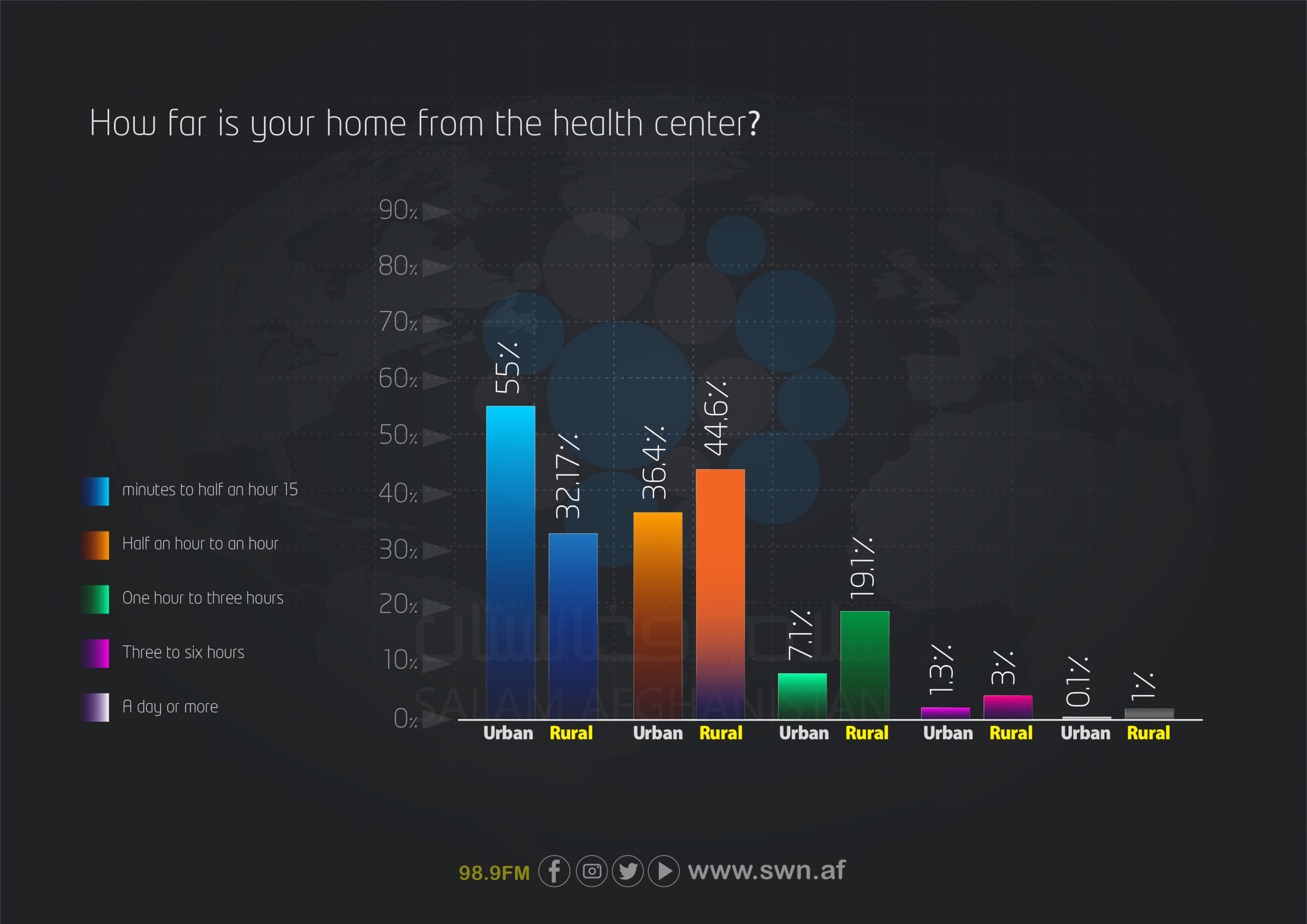
In terms of travel time to healthcare centers, most urban residents (55%) are located within 15 minutes to half an hour, whereas in rural areas, this figure is only 32.17%. The largest group in rural areas (44.6%) takes between half an hour and one hour to reach a healthcare center. Additionally, 19.1% of rural residents spend more than one hour traveling, compared to only 7.1% in urban areas.
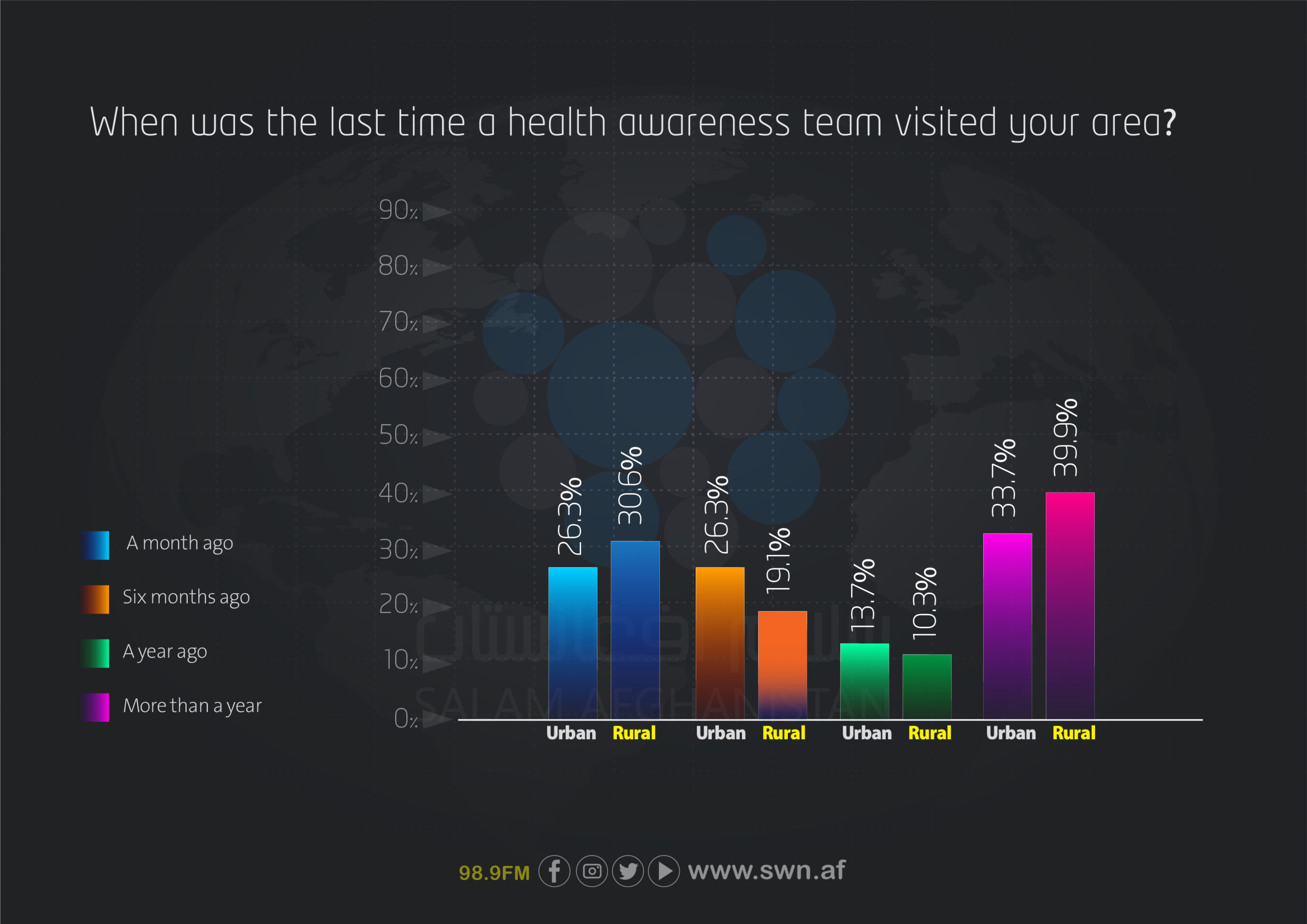
Regarding the presence of health awareness teams, most rural respondents (39.9%) stated that it has been over a year since the last visit of an awareness team, compared to 33.7% in urban areas. In rural areas, only 30.6% reported that an awareness team had visited their area within the past month, indicating relatively limited efforts in providing health awareness services to rural communities.
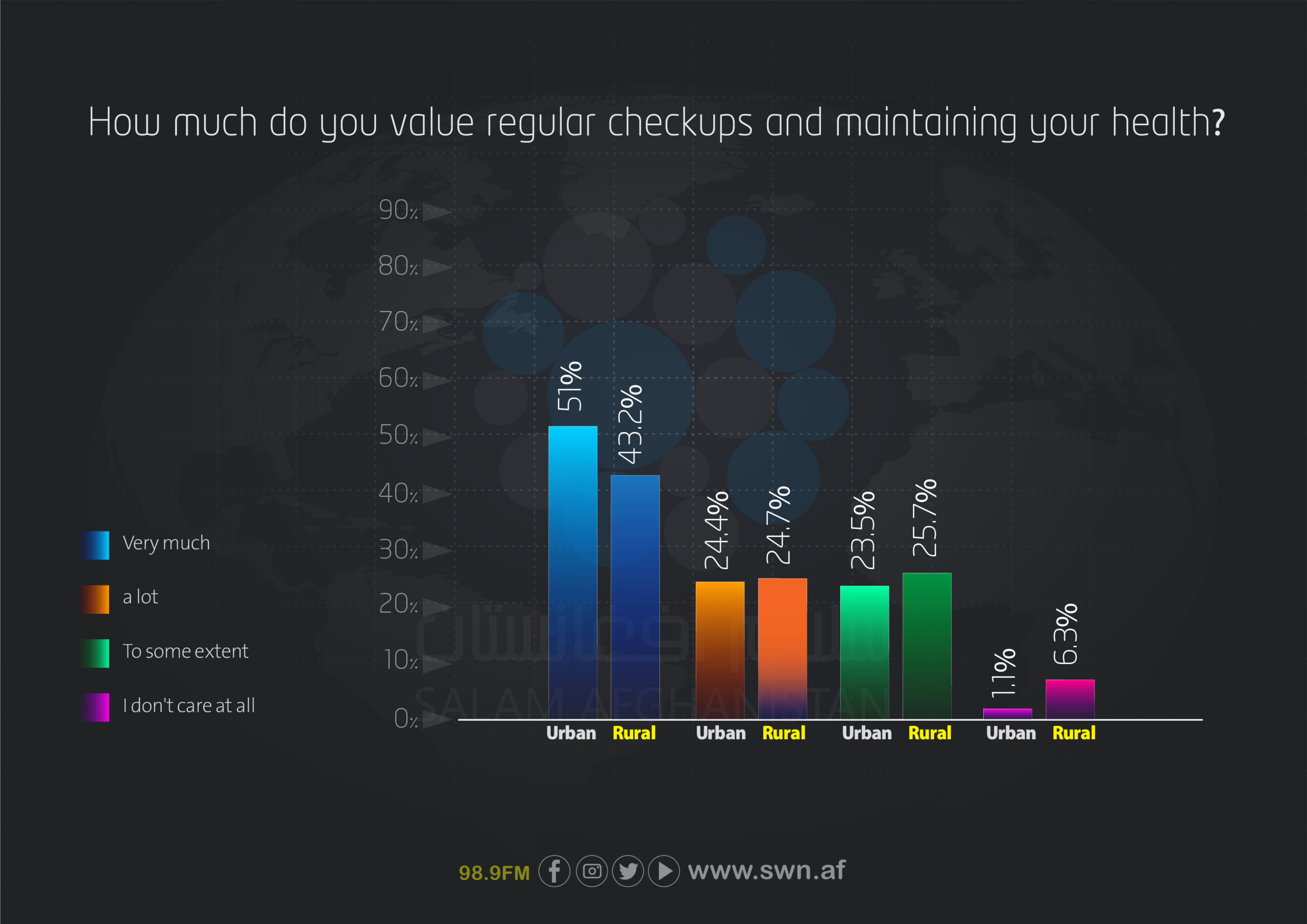
Finally, the importance placed on regular health check-ups among urban and rural respondents is also comparable. Among urban residents, 51% reported valuing their health “very much,” compared to 43.2% of rural residents. The percentage of individuals who do not value check-ups at all is higher in rural areas (6.3%) than in urban areas (1.1%), indicating the need to increase awareness and access to preventive services in rural communities.
Key highlights
- Service Quality: Over 80% of rural and 75% of urban respondents rated healthcare as poor or below average.
- Lack of geographic access: Nearly 78% of rural residents need between more than one hour and up to a full day to reach healthcare centers. Unpaved, rough, and sometimes impassable roads pose a serious barrier to timely access to emergency care.
- Shortage of medicines: 87% of rural residents face a shortage of medicines, while 10% are completely deprived of access to them.
- Crowding & Waiting Times: 68% of urban patients wait more than one hour to receive services, indicating weak capacity and inefficiency in healthcare delivery.
- Lack of awareness programs: 40% of rural residents reported that no health awareness team has visited their area for over a year.
- Lack of service diversity and dependence on governmental centers:9% of rural residents rely solely on governmental centers and have no access to private options, which undermines competition and service quality.
- Low attention to personal health: 56.8% of rural respondents do not give adequate attention to their health, and 6.3% do not engage in any preventive care.
Key recommendations
A comprehensive, urgent, and field-data–driven plan is needed to:
- Establish local healthcare centers in remote areas
- Reform the distribution system of medicines
- Improve rural roads leading to healthcare centers
- Restart health awareness programs
- Increase access to private healthcare services by encouraging local investment
Conclusion
The current state of Afghanistan’s healthcare system is alarming and requires immediate structural review and intervention. Delays in addressing these challenges could have serious human and social consequences. A comprehensive approach to improving infrastructure, securing resources, raising awareness, and expanding services is essential to ensure public health nationwide.
Researcher and Author: Halima Nazari
Translated by: Friba Qaderi




